Approximately one in eight adults in the United States has now used a GLP-1 receptor agonist — drugs like Ozempic and Wegovy — for weight loss. Yet more than half of those who start the medication discontinue it within 24 months, and many later restart. A new preclinical study from the Perelman School of Medicine at the University of Pennsylvania, published on 28 April 2026 in the Journal of Clinical Investigation Insight, reveals that this stop-and-start pattern may be significantly undermining the drugs' effectiveness — and the biological reason is more surprising than most patients and clinicians expect.
The Study: What Happens When You Stop and Restart
Thomas H. Leung, MD, PhD, the Herman Beerman Professor in Dermatology at Penn, and his colleagues studied two groups of overweight mice over a four-month period. The first group received the GLP-1 drug semaglutide (the active ingredient in Ozempic and Wegovy) consistently for the entire study. The second group followed a stop-and-start cycle: two weeks on the drug, two weeks off, for three cycles, before switching to consistent use for the final two months.
Both groups showed similar weight loss in the first two weeks. But from that point, the trajectories diverged dramatically. The stop-and-start group rapidly regained weight during every "off" period. Crucially, when they restarted the drug, they were unable to return to their previous lowest weight. Even after 62 days of consistent use at the end of the study, the intermittent group remained 20 percent heavier than the consistent group.
"The effectiveness of these medications may depend heavily on consistency. Taking GLP-1s may be one of those decisions that people need to discuss and make with their doctor, knowing that taking the drug requires a long-term commitment." — Thomas H. Leung, MD, PhD, Penn Medicine
The Muscle Floor: Why Each Restart Works Less
The researchers used MRI to track body composition throughout the study, and this is where the most important finding emerged. Weight loss from GLP-1 drugs typically consists of approximately 40 percent muscle and 60 percent fat. However, when a patient stops the drug and regains weight, they almost exclusively regain fat — not muscle.
By the time a patient restarts the medication, their muscle-to-fat ratio has shifted significantly. The body appears to reach what the researchers call a "muscle floor" — a biological threshold below which it will not allow further muscle loss. Once muscle percentage hits this low point, the body resists further weight loss to protect itself.
| Group | Weight at End of Study | Muscle Mass | Fat Mass | Outcome |
|---|---|---|---|---|
| Consistent semaglutide | Baseline − 15% | Preserved | Significantly reduced | Sustained weight loss |
| Stop-start semaglutide | Baseline − 5% | Significantly reduced | Regained almost exclusively as fat | 20% heavier than consistent group |
Table 1: Body composition outcomes after 4 months in consistent vs. stop-start GLP-1 groups (preclinical mouse model).
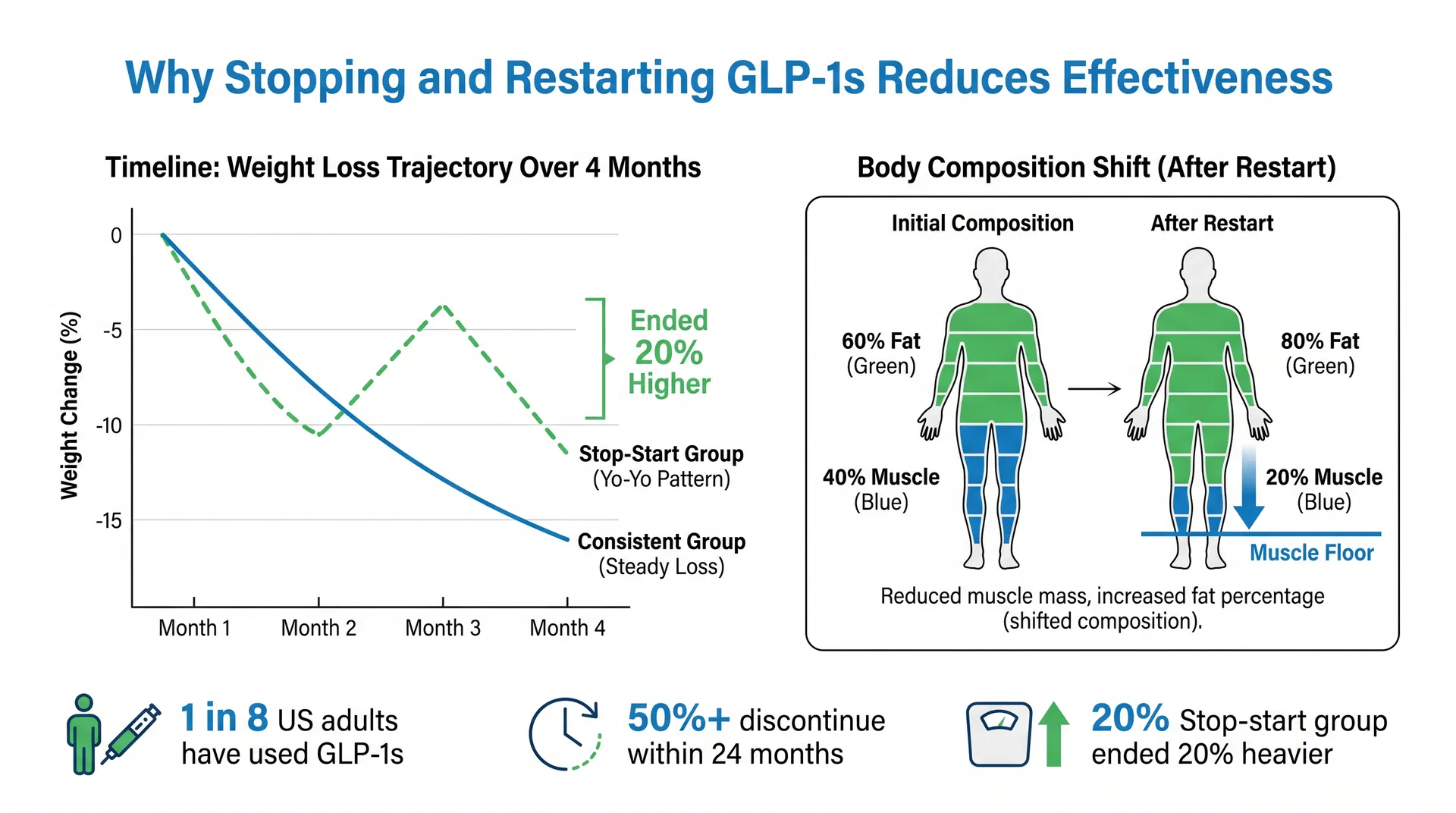
Figure 1: Left — the stop-start group shows a yo-yo weight pattern, ending 20% heavier than the consistent group. Right — after restarting, the body composition shifts from 40% muscle / 60% fat to 20% muscle / 80% fat, triggering the muscle floor effect.
The Minoxidil Parallel
Leung draws an instructive analogy to minoxidil, the hair-regrowth medication. Minoxidil is well-known to show diminishing returns when used inconsistently — patients who stop and restart the drug often find it less effective on subsequent courses. GLP-1s appear to fall into the same pharmacological category: drugs whose effectiveness is intrinsically tied to continuous use.
"Since stopping and starting is so common, my colleagues and I thought it was worth investigating whether or not the GLP-1s work as well each time," Leung said. The answer, at least in this preclinical model, is clearly no.
What This Means for Patients and Clinicians
The findings have several immediate clinical implications:
1. Muscle preservation is critical during GLP-1 therapy. Because weight regain after stopping the drug is almost entirely fat, patients who cycle on and off the medication progressively worsen their muscle-to-fat ratio. Clinicians should proactively counsel patients on resistance exercise and adequate protein intake to preserve muscle mass, both during treatment and during any planned breaks.
2. Discontinuation decisions should be made carefully. The study suggests that patients who are considering stopping GLP-1 therapy — whether due to cost, side effects, or personal preference — should understand that restarting may not produce the same results as the initial course.
3. The findings need human validation. The study was conducted in mice, and the researchers are explicit that the results need to be confirmed in human clinical trials. The muscle floor hypothesis is biologically plausible but has not yet been directly demonstrated in people.
4. The question extends to tirzepatide. Future research will need to investigate whether the same diminishing-returns effect applies to tirzepatide (Zepbound), which targets both GLP-1 and GIP receptors and has shown even greater weight-loss efficacy than semaglutide alone.
The Broader Context: A Medication Requiring Long-Term Commitment
The study lands at a moment when GLP-1 drugs are reshaping medicine at scale. The FDA approved a higher dose of Wegovy in 2026, and Boehringer Ingelheim's dual glucagon/GLP-1 agonist survodutide recently reported 16.6% weight loss in a Phase 3 trial. The pipeline of next-generation obesity drugs is robust.
But the Penn Medicine findings serve as an important counterweight to the enthusiasm: these are not drugs that can be taken intermittently like a pain reliever. They appear to require the same kind of long-term commitment as statins or antihypertensives — medications that work best when taken every day, indefinitely.
For the millions of people who have started and stopped GLP-1 therapy, the message is not one of despair but of informed decision-making. Understanding the muscle floor effect, and the importance of exercise and nutrition in preserving muscle mass during treatment, may be the difference between a therapy that transforms a patient's health and one that produces a frustrating cycle of partial results.
Source: Penn Medicine / Perelman School of Medicine, University of Pennsylvania. Published in Journal of Clinical Investigation Insight, April 28, 2026. Lead investigator: Thomas H. Leung, MD, PhD.